delta dental appeal form
How to Know When You Can Appeal When Delta Dental. Delta Dental requires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical corrections or to provide additional information to support the.

A Guide To Dental Claim Denials Ajust
General Correspondence Claims.

. The Appeal Request Form must be received by Delta Dental DDKS within 180 calendar days from the date of the original adverse benefit determination or the corresponding remittance. Mail Inquiries for Delta Dental PPO Plan. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX.
Questions about the appeals process you may call the Departments Consumer Assistance Office at 602 3642499 or 8003252548. Denial of services or where we only approved part of a service. ASO contract addendum for HIPAA privacy and security.
This form is not needed for. Appeals Grievances Delta Dental of Arizona Appeals Grievances Who should we respond to. 6 Reasons to choose a PPO Delta Dental PPO and Premier.
Orthodontic benefits Go paperless Re-credentialing forms Enterprise standard credentialing form CO credentialing form NC. To submit an appeal complete the form in its entirety and attach all documents records and any other information related to the claim. Delta Dental HIPAA Form 14b ASO Groups.
DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist. An Appeal is a request for a review of an action by Delta Dental. Use this form to update the status of your practice as a DeltaCare provider.
An Appeal can be for any of the following. THE PO BOX IS FOR CLAIMS ONLY. Delta Dental HIPAA Form 14a Risk Groups.
Submit a credentialing or recredentialing application online with App Central DDMA Provider web portal Important Forms Direct Deposit Form W-9 from the Internal Revenue Service Individual. Delta Dental of California Federal Government Programs PO Box 537007 Sacramento CA 95853-7007. List all documents you submit with your appeal in the.
Under the guidance of the California Department of Health Care Services the Medi-Cal Dental Program aims to provide Medi-Cal members with access to high-quality dental care. Healthy Smile Healthy You enrollment. First Name Last Name Street Address City State Zip Code Email Phone Patient.

Delta Dental Of Oregon Forms For Members

Forms Delta Dental Of Iowa

Delta Dental Of Oregon Forms For Members
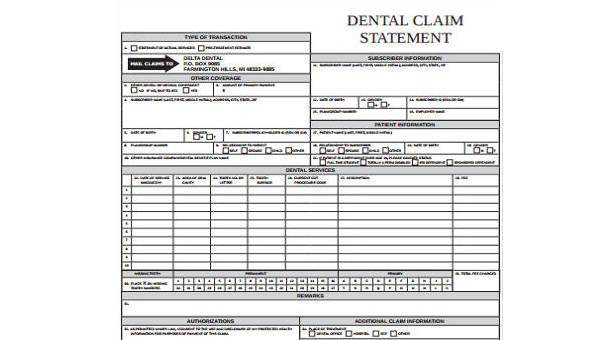
Free 8 Dental Claim Forms Samples In Ms Word Pdf

Sample Letters Of Appeal To Dental Insurance Lovetoknow
![]()
Understanding Your Explanation Of Benefits Eob Delta Dental Of Illinois

Claim And Administrative Forms Delta Dental
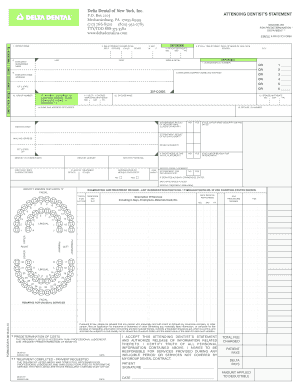
Delta Dental Printable Claim Form Fill Online Printable Fillable Blank Pdffiller
Forms And Resources Delta Dental Of Ohio

Dental Insurance Forms Delta Dental Of Washington

Delta Dental Of Minnesota Complaints Better Business Bureau Profile

News Release Delta Dental Of Wisconsin

How Are Dental Claims Handled Delta Dental Of Illinois

Hawk I Orthodontic Network Forms Delta Dental Of Iowa
Forms And Resources Delta Dental Of Michigan

Delta Dental Goes Mockumentary Style For Long Live Smile Power

Delta Dental Of Arkansas Claims Address Fill Online Printable Fillable Blank Pdffiller
Does Delta Dental Cover Clear Aligners Braces
Delta Dental Michigan Appointment Of Representative Forms